Guest Blog Post by Rachel Wynn, MS CCC-SLP  It has been about three years since I completed graduate school. As a student, I learned a lot in graduate school and during my leveling courses; however, I have learned far more in the three years following graduation. There isn’t space in this blog post to explain everything I’ve learned. So today, I’m going to share the three things I learned that made the biggest impact on how I deliver care in general.
1. People should come before profits. I remember the ethics lectures in graduate school. It seemed so common sense to me. I figured these ethical dilemmas would happen occasionally. I’ve got a good head on my shoulders and a strong desire to advocate for social justice. Of course, people come before profits. Not all companies and facilities consistently act on the belief people come before profits. It’s a frequent complaint in the community of therapists working in healthcare that productivity expectations seem to be more important than patient outcomes. I highly recommend joining some of the Facebook forums (Adult Rehab Speech Therapy and Slpeeps) and reading some of the discussions about ethics. Just search for “ethics” or “productivity” within the forum. Having this awareness going into your interviews and first positions will be very helpful. Learn more: ASHA’s Employer Demands in Healthcare and Good Work Conditions for Therapists 2. You have to meet people with dementia where they are. Dementia is a progressive disease. Whether or not people and their families have insight into deficits or are living in denial, we have to meet them where they are. We meet them in their confusion and delusions. Meeting people with dementia where they are sometimes involves lying, and that’s okay. I frequently talk to family members about lying versus rationalizing. Many people want to always tell the truth and rationalize with family members. When people say they want to go home, families may try to rationalize that they are home. They live here now, etc. This is the wrong approach. A better approach is to validate the person’s concern then distract. “Let’s eat dinner before you go home.” Validation can be calming. We all want to heard. Then distraction can set in. The key is to communicate in a way that resolves the problems and concerns that people with dementia feel they are experiencing. I had a patient that told me she had no time for my therapy tasks. She had too many things to do. She felt she needed to be productive. She was agitated by continued attempts, so I set up a calendar system with her and her personal caregiver and put speech therapy on her calendar. The next day I arrived at my scheduled appointment and had specific tasks for us to do that weren’t standard therapy. She followed directions and completed problem solving in making holiday cards. Then we worked on walking safely with her walker when we delivered the cards. It worked wonderfully. I heard her, validated her concerns, and met her where she was. Learn more: Eden Alternative Equals Better Care for Elders and An Amazing Village Designed Just for People With Dementia 3. People die. Death is the ultimate rite of passage. Many people fear death. People and their families need someone to tell them they have choices. SLPs have an expertise in dysphagia that can help families make choices. Death isn’t a prescribed process. Respecting patient and family wishes at end of life is the best thing we can go to help them experience a good death. I’ve worked with people who are at end of life and their bodies and mind are beginning to shut down. Some families want to fight until the very last moment. Terminal cancer in a 90-year-old beginning to experience multi-organ failure is just a reason to fight harder. After seeing families go through this, I have clearly communicated to my family members that this is not what I want. I had an end of life and quality of life talk with a family recently. Sometimes, I feel a bit like the Grimm Reaper, because I enjoy these conversations. (They used to make me uncomfortable.) Death is certain, but I feel like I can do my part to empower the family and patient to experience a good death. If they don't want thickened liquids, I can provide recommendations to make them as comfortable as possible with thin liquids. My job isn't always to prevent illness and death, sometimes the only focus is improving quality of life. What an incredible honor! Learn more: Check out ASHA’s Patient Rights and Patient Choices. Special Thanks to Rachel Wynn for writing a great blog post with her perspective pertaining to the geriatric population! Rachel Wynn, MS CCC-SLP is speech-language pathologist specializing in geriatric care. She blogs at Gray Matter Therapy, which strives to provide information about geriatric care including functional treatment ideas, recent research, and ethical care. Rachel’s projects include: Gray Matter Therapy Newsletter, Research Tuesday, and Patient and Family Education Handouts. Find her coaching new SLPs, on Facebook, on Twitter, or hiking with her dog in Boulder, CO.
3 Comments
Below is a brief overview to describe types of strokes. I am a visual learner, so I created some pictures to describe each type of stroke. On The National Stroke Association’s website http://www.stroke.org/site/PageServer?pagename=type at the bottom of the page, there are two animations to show hemorrhagic and ischemic strokes. They also provide more in depth information regarding each type of stroke. http://www.mind.ilstu.edu/usersSys/courses/courseHomepage.php?courseGUI=75 I highly recommend exploring this website after you review the different types of strokes. It is a Virtual Stroke Lab that provides you with patient data, protocols and it is very interactive! I have to admit I enjoyed the lab myself and after there are quizzes. http://www.mind.ilstu.edu/curriculum/virtual_stroke_lab/stroke_student_handout.pdf This is the virtual handout to accompany the Virtual Stroke Lab. 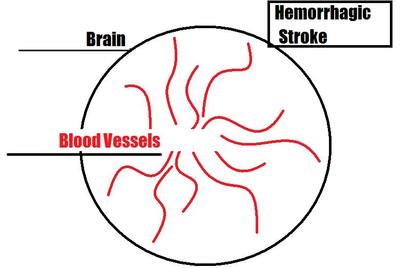 Hemorrhagic stroke occurs when a blood vessel in the brain bursts and blood bleeds into the brain. 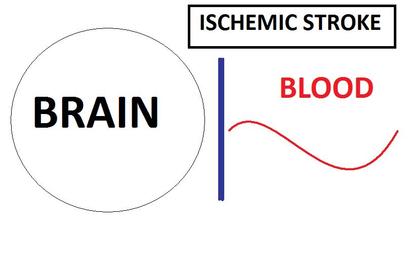 Ischemic stroke occurs when blood is blocked from getting to the brain. 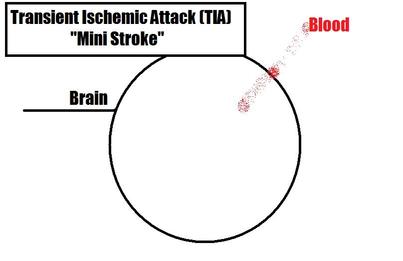 A Transient Ischemic Attack (TIA) is also known as a “mini stroke” because it happens for a small amount of time when not enough blood flows to the brain. This is a great link to a handout that provides more information on Transient Ischemic Attack (TIA), it also explains the difference between TIAs and strokes. http://www.annals.org/site/intheclinic/itc-transient-ischemic-attack-patient-information.pdf |
 This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License. |
© Copyright 2010-2020 futureslps.com All Rights Reserved Worldwide